

FIRST TRIMESTER SCREENING
When is it done?
The optimal time for doing a combined first trimester screening is from 11 weeks to 13 weeks 6 days. The CRL should be a minimum of 45 mm to a maximum of 84 mm.
Why 11 - 13+6?
1. Prediction of risk from NT is best from 11 weeks onwards and NT regresses by 14 weeks.
2. The biochemistry markers that are used for first trimester screening are free b-hCG and PAPP-A these are most sensitive between 9 - 11 weeks.
The process
Step 1: Maternal age related risk – A priori risk
Step 2: Measure NT correctly
Step 3: Use appropriate software for recalculating the risk for a specific NT. If Biochemical testing is also done (free beta- hCG & PAPP-A), incorporate it into the software and predict combined risk
The process of screening involves taking note of some maternal criteria. These include
· Maternal age (date of birth)
· Maternal weight
· Parity
· Method of conception (natural/ assisted)
· Ethnicity
· Smoking
At the 11 - 13 week scan the following are noted.
Accurate dating of pregnancy is the first step to the process of screening. This is either established by an earlier scan or at the time of the 11 - 13 weeks scan by taking an accurate CRL. As interpretation of NT is based on CRL, it is important that the CRL is taken in the standard position and the baby is not too flexed or extended when the measurement is taken.
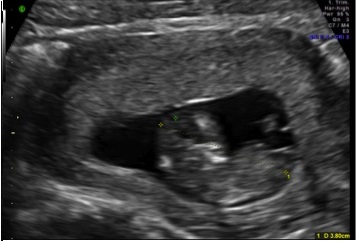
figure: flexed fetus wrong CRL

figure: neutral position correct CRL
NUCHAL TRANSLUCENCY
Nuchal translucency is the sonographic appearance of subcutaneous accumulation of fluid behind the fetal neck in the first trimester of pregnancy. The term translucency is used, irrespective of whether it isseptated or not and whether it is confined to the neck or envelopes the whole fetus. The incidence of chromosomal and other abnormalities is related to the size, rather than the appearance of NT.
Fetal NT increases with gestation. For given CRL, each NT gives a likelihood ratio. Each NT value for a specific CRL has a likelihood ratio (LR) and larger the NT, higher the LR. An NT > 3.5mm is above the 99th centile and warrants direct testing.
The Nuchal translucency measurement is to be taken according to the FMF specifications.

figure: increased NT
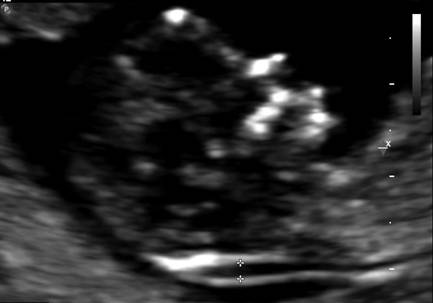
figure: NT measurement
Nuchal Translucency Measurement
· A mid-sagittal section of the fetus should be obtained and the NT should be measured with the fetus in the neutral position.
· Only the fetal head and upper thorax should be included in the image. The magnification should be as large as possible and always such that each slight movement of the calipers produces only a 0.1 mm change in the measurement.
· The maximum thickness of the subcutaneous translucency between the skin and the soft tissue overlying the cervical spine should be measured. Care must be taken to distinguish between fetal skin and amnion.
· The calipers should be placed on the lines that define the NT thickness – the crossbar of the caliper should be such that it is hardly visible as it merges with the white line of the border and not in the nuchalfluid.
· During the scan, more than one measurement must be taken and the maximum one should be recorded.
Biochemistry
This involves a simple blood test which measures the free beta- hCG and PAPP-A. The level of free b-hCG in maternal blood normally decreases with gestation. The level of PAPP-A in maternal blood normally increases with gestation. In trisomy 21 pregnancies free b-hCG is increased, and PAPP-A level is decreased.
For a given gestation, each b-hCG and PAPP-A level represents a likelihood ratio that is multiplied by the priori risk to calculate the new risk. The higher the level of b-hCG and the lower the level of PAPP-A the higher the risk for trisomy 21.
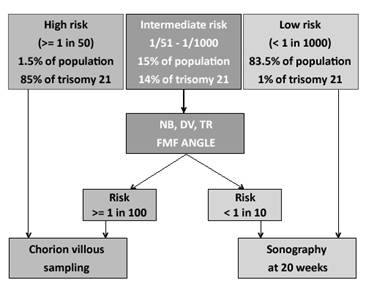
Use of additional markers
· These markers are used to predict risk of Trisomy 21 in the boderline risk category ( defined as a risk of 1: 51 to 1: 1000) and include Nasal bone - absent in 60 - 70% trisomy 21
· DV / TR - Ductus venosus abrnomalities are seen in 80% of Trisomy 21 and 5% of normal fetuses.
The FMF algorithm
The next step
When a result of screening comes back as screen negative, no further testing is generally warranted because it suggests a ‘low risk’ of having a baby with Down syndrome. When a woman screens positive, it does not mean that the baby is affected. This only puts her in a higher risk group and further invasive testing is offered for fetal karyotyping.
Advantage of First trimester screening
The advantages of first-trimester screening extend beyond the observed higher detection rates. The main advantage for the majority of women is the earlier reassurance provided to those with ‘low-risk’ results. Those who are screen positive can have a CVS and diagnosis by the 14th week. Furthermore, for those who choose to terminate an aneuploid pregnancy, decisions can be made early and social issues can be handled better. Complication rates are also lower at earlier gestations.
Advantages of the 11 - 13 week scan
The first-trimester nuchal translucency scan offers several additional benefits.
A range of abnormalities other than aneuploidy have been associated with increased nuchal translucency. These include cardiac anomalies, diaphragmatic hernia, skeletal dysplasia, and abnormal lymphatic drainage associated with neuromuscular disorders. Therefore, identification of an increased nuchal translucency measurement should prompt not only a diagnostic test for aneuploidy, but also a thorough anatomic survey for structural anomalies and a detailed fetal echocardiogram in the case of a normal karyotype.
A significant number of anomalies can be picked up at this gestational age. With the increasing use of higher resolution machines a detailed anatomical survey can be done at the 11- 13 week scan.
ICOGU
CUSP XIV
What is the minimum duration for training in OB/GYN ultrasound?
View Results
